Table of Contents >> Show >> Hide
- What does “pacemaker for heart failure” really mean?
- How do pacemakers for heart failure work?
- Who can benefit from a pacemaker for heart failure?
- Who may not benefit as much?
- What benefits can a heart failure pacemaker provide?
- What is the implantation procedure like?
- What are the risks and downsides?
- What is recovery like after getting a pacemaker for heart failure?
- Living with a CRT device day to day
- Questions to ask before getting a pacemaker for heart failure
- Final thoughts
- Real-life experiences and what patients often notice over time
- SEO Tags
Note: This article is for educational purposes only and is not a substitute for personal medical advice, diagnosis, or treatment.
When people hear the word pacemaker, they often picture a tiny device that simply keeps a slow heart from taking too many coffee breaks. That is true for many standard pacemakers. But when it comes to heart failure, the story is a little more specialized and much more interesting.
In heart failure, the problem is not always that the heart is beating too slowly. Sometimes the bigger issue is terrible timing. The heart’s lower chambers may squeeze out of sync, turning each heartbeat into a clumsy group project. In those cases, a special kind of pacemaker can help the heart pump in a more coordinated way. This treatment is called cardiac resynchronization therapy, or CRT. You may also hear it called a biventricular pacemaker.
CRT is not for everyone with heart failure, and it is not the first step for every patient. But for the right person, it can reduce symptoms, improve quality of life, lower the risk of hospitalization, and help the heart work more efficiently. The key is understanding who is most likely to benefit, how the device works, and what life looks like after implantation.
What does “pacemaker for heart failure” really mean?
A traditional pacemaker usually treats bradycardia, which means a heart that beats too slowly. It sends small electrical impulses to keep the heartbeat from dragging its feet. For heart failure, though, doctors are often talking about CRT, not just a standard single-chamber or dual-chamber pacemaker.
A CRT device is designed to help the heart’s ventricles contract together. That matters because many people with heart failure with reduced ejection fraction have an electrical delay, often seen on an ECG as a left bundle branch block or another wide QRS pattern. In plain English, the heart muscle is not firing in a smooth, coordinated way. The result is less effective pumping, more symptoms, and a heart that has to work harder than it already does.
This is why a biventricular pacemaker is different from a standard pacemaker. It is not just setting the pace. It is fixing the rhythm of the teamwork between the two lower chambers. Think of it less like a whistle and more like a conductor telling an unruly orchestra when to come in.
How do pacemakers for heart failure work?
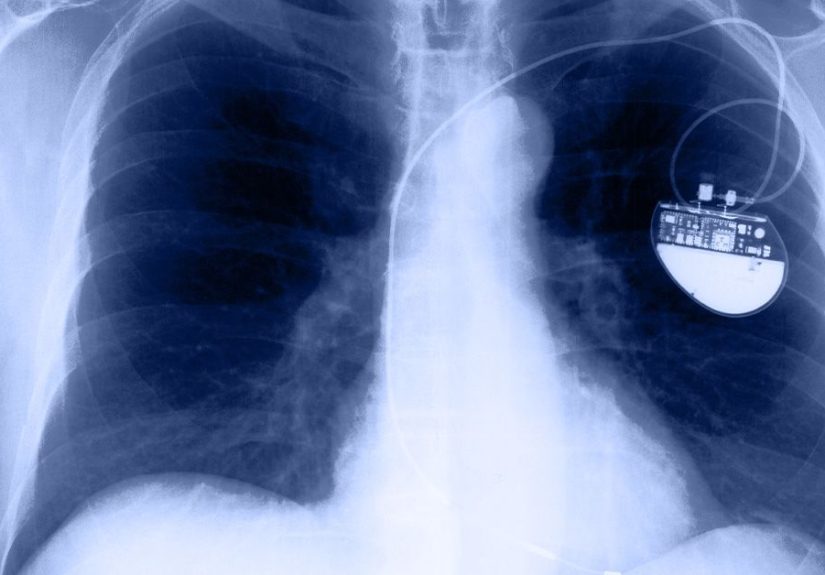
A heart failure pacemaker usually has a small pulse generator placed under the skin near the collarbone. It is connected to leads, or thin wires, that carry electrical signals to the heart. In a typical CRT device, there are three leads: one to the right atrium, one to the right ventricle, and one positioned to stimulate the left ventricle.
The device sends tiny electrical impulses that help both ventricles beat at nearly the same time. That better coordination can improve how efficiently the heart pumps blood to the lungs and body. For patients whose symptoms are driven in part by electrical dyssynchrony, this can make a real difference.
There are two main versions:
CRT-P
This stands for cardiac resynchronization therapy with pacing. Its main job is to resynchronize the heartbeat and support pumping.
CRT-D
This combines CRT with an implantable cardioverter-defibrillator. In addition to resynchronizing the heart, it can detect dangerous ventricular arrhythmias and deliver therapy, including a shock if needed. This option may be chosen when a patient also has a meaningful risk of sudden cardiac death.
Standard pacemakers and even leadless pacemakers still have important roles in cardiology, but they are not usually the go-to answer for classic heart failure-related dyssynchrony. In selected patients, doctors may also use newer approaches such as His bundle pacing or left bundle branch area pacing, which aim to activate the heart’s natural conduction system more directly.
Who can benefit from a pacemaker for heart failure?
This is the million-dollar question, minus the million-dollar co-pay. The people most likely to benefit are usually those with symptomatic heart failure despite guideline-directed medical therapy, especially if testing shows reduced pumping function and delayed electrical activation.
In general, the strongest candidates are people who have:
- Heart failure with reduced ejection fraction, often an ejection fraction of 35% or lower
- Ongoing symptoms such as fatigue, shortness of breath, or exercise intolerance despite appropriate medications
- A wide QRS complex on ECG, especially with left bundle branch block
- Evidence that the ventricles are not contracting together
Patients with LBBB and a QRS duration of 150 milliseconds or more tend to get the clearest benefit. Some patients with a QRS between 130 and 149 milliseconds may also be considered, especially if they have LBBB. Others with non-LBBB patterns may still be candidates, but the expected benefit can be less predictable.
CRT may also help some people with atrial fibrillation, particularly if doctors can ensure a very high percentage of biventricular pacing. In some cases, that may require additional rhythm management steps. Another group that may benefit includes people who need frequent right ventricular pacing because of heart block. In the wrong setting, long-term right ventricular pacing alone can worsen heart failure, so a more synchronized pacing strategy may be preferred.
Who may not benefit as much?
Not every person with heart failure needs a pacemaker, and not every pacemaker candidate will be a CRT candidate. In fact, some patients are better treated with medications alone, some need different devices, and some need evaluation for advanced heart failure therapies.
CRT is generally less helpful for people who have:
- Mild symptoms without clear electrical dyssynchrony
- Diastolic heart failure or heart failure with preserved ejection fraction, unless there is another specific pacing reason
- Ventricles that already beat together
- Acute decompensated heart failure that has not yet been stabilized
- Active infection, sepsis, or serious bleeding risk
- Severe noncardiac illness that limits life expectancy
Response also varies. Some patients improve dramatically, while others improve modestly, and a minority do not respond as hoped. That does not mean the device “failed” in a simplistic sense. Heart failure is complex, and outcomes can depend on lead position, scar tissue in the heart, atrial fibrillation burden, medication optimization, and the exact electrical pattern on the ECG.
What benefits can a heart failure pacemaker provide?
For the right patient, the benefits can be meaningful and sometimes life-changing. CRT does not “cure” heart failure, but it can make the heart pump more efficiently and reduce the burden of symptoms.
Potential benefits include:
- Less shortness of breath
- Better exercise tolerance
- Improved quality of life
- Fewer hospitalizations for heart failure
- Improved ejection fraction in many responders
- Better coordination of the heart’s pumping action
- In some patients, improved survival
These improvements do not always happen overnight. Some patients feel better within weeks, while others notice changes gradually over several months. Follow-up visits are important because doctors often adjust device settings after implantation to help the therapy work better.
What is the implantation procedure like?
The phrase “minor surgery” sounds comforting until it is your chest involved, but CRT implantation is a routine procedure for experienced electrophysiology teams. It is usually done in a hospital or specialized cardiac center.
During the procedure, the doctor makes a small incision near the collarbone and threads the leads through a vein into the heart using imaging guidance. The leads are connected to the device generator, which is placed under the skin. Patients are often awake with local anesthesia and sedation, though the exact approach varies.
The procedure may take a few hours. Many patients stay overnight for monitoring, then go home the next day if everything looks good. Before discharge, the team checks the device, reviews wound care, and explains activity restrictions.
What are the risks and downsides?
No implanted heart device comes with a magic wand and zero trade-offs. While CRT implantation is common and generally safe, it still involves real risks.
Possible complications include:
- Infection at the implant site
- Bleeding or bruising
- Collapsed lung
- Lead dislodgement
- Heart perforation or fluid around the heart
- Device malfunction
- Diaphragm or nerve stimulation that causes twitching or hiccup-like sensations
- The need for another procedure to reposition or replace a lead
There is also the reality that some people simply do not experience major improvement. That can be frustrating, especially when expectations are sky-high. Good pre-implant evaluation helps, but medicine is not a vending machine: you do not always insert a lead and get perfect results every time.
What is recovery like after getting a pacemaker for heart failure?
Recovery is usually measured in weeks, not months, though full adjustment to the therapy can take longer. The incision may feel sore for a few days, and patients are typically told to avoid heavy lifting, vigorous upper-body movement, and raising the arm on the implant side too much for several weeks.
Many people return to light daily activity within a few days. More strenuous activity may need to wait until the leads have settled securely in place. Follow-up visits are essential to check healing, review symptoms, and fine-tune device settings.
Long term, the device battery lasts several years and is monitored regularly. Replacement is usually simpler than the first implantation because the leads often stay in place if they are working properly.
Living with a CRT device day to day
Daily life after implantation is often more normal than people expect. Most home appliances are fine. Travel is usually possible. CT scans are generally still possible, and many modern devices are MR-conditional, meaning MRI may be allowed under specific conditions. The important word there is “specific,” not “surprise road trip to the scanner.”
Patients should also know that strong magnets can interfere with device function. Phones, smart watches, and other magnetic electronics should not be kept directly over the device. A simple rule many clinicians repeat is to keep such electronics at least six inches away from the implant site.
People with a CRT-D may have extra emotional adjustment because the device can deliver a shock if a dangerous rhythm occurs. Some patients feel safer knowing that protection is there. Others feel anxious waiting for a shock that may never come. Both reactions are understandable, and both deserve honest conversation with the care team.
Questions to ask before getting a pacemaker for heart failure
If you or a loved one is considering CRT, a good discussion with the cardiology team matters. Helpful questions include:
- Am I a candidate for CRT-P, CRT-D, or a different pacing strategy?
- What is my ejection fraction, and what does my ECG show?
- Do I have left bundle branch block or another wide QRS pattern?
- Have my medications been optimized first?
- What improvement should I realistically expect?
- What are the risks in my case?
- How often will the device need to be checked?
- Will I need remote monitoring?
- Are MRI scans allowed with this device?
Final thoughts
A pacemaker for heart failure is not a one-size-fits-all gadget. For many patients, it specifically means cardiac resynchronization therapy, a device that helps the heart’s lower chambers beat together when poor electrical timing is making heart failure worse.
The people most likely to benefit are those with reduced ejection fraction, persistent symptoms despite the right medicines, and clear electrical dyssynchrony, especially left bundle branch block. For these patients, CRT can improve symptoms, reduce hospital visits, and help the heart pump in a more organized way.
The trick is proper selection. A pacemaker is not automatically the answer for every patient with heart failure, but for the right person, it can be one of the most useful tools in the toolbox. And when your heart’s timing has gone completely off-script, getting the beat back in sync can make an enormous difference.
Real-life experiences and what patients often notice over time
One of the most common experiences people describe before getting a heart failure pacemaker is sheer frustration. They may already be taking multiple medications, trying to watch salt, tracking weight, and doing all the “good patient” things, yet they still feel winded walking across a room or climbing a short flight of stairs. Many say they are less bothered by chest pain than by the constant fatigue. It can feel like the battery in their body never charges past 20%.
After the cardiologist explains that the issue may not be just weak pumping, but also poor electrical timing, patients often feel equal parts relief and confusion. Relief, because there is a possible next step. Confusion, because the word “pacemaker” sounds simple, while “cardiac resynchronization therapy” sounds like something invented by a committee with a caffeine problem. Once it is explained clearly, though, many patients latch onto the idea that their heart is not just weak; it is out of sync.
On procedure day, a very common experience is nervous anticipation. Even patients who have had prior heart procedures often say this one feels emotionally different because a device will stay with them long term. Most are surprised that the implantation is less dramatic than they feared. Soreness around the incision, a pulling sensation near the collarbone, and limited arm movement are frequent early complaints. For the first week or two, many people say sleeping comfortably is more annoying than painful.
In the first month, improvement is often gradual rather than cinematic. Some patients do not feel dramatically different right away and worry that the device is not working. That is a normal fear. In reality, the heart may need time to remodel, medications may still need adjustment, and device settings may need fine-tuning. Follow-up appointments matter more than people expect. A small programming change can sometimes make a noticeable difference in symptoms.
Patients who respond well often describe a similar pattern: less shortness of breath, more stamina, and a little more confidence doing ordinary things. They may notice they can walk farther, recover faster after activity, or sleep flatter without feeling breathless. For some, the change is dramatic. For others, it is more subtle but still meaningful. Being able to grocery shop without sitting down halfway through can feel like winning an Olympic medal, just with fewer cameras.
There are also emotional experiences that do not always get enough attention. Some people feel reassured by having a device. Others feel self-conscious about the bump under the skin or anxious about depending on hardware. Patients with a CRT-D may be especially worried about shocks. Honest counseling helps. So does meeting others who have been through it and learning that life with a device is usually far more ordinary than it sounds at diagnosis.
Not every story is a huge success, and it is important to say that plainly. Some patients improve only a little. Some need lead revisions or additional rhythm management. Some continue to have advanced heart failure symptoms and eventually need more intensive therapies. Still, even in those cases, the device may be one important part of a broader treatment plan rather than a failed experiment.
In the end, the most consistent patient experience is this: good outcomes depend on more than the implant itself. The best results usually happen when the device is matched to the right patient, medications are optimized, follow-up is steady, and expectations are realistic. A pacemaker for heart failure is not magic, but for many patients, it can help life feel bigger again.






