Table of Contents >> Show >> Hide
- What is opioid use disorder?
- How common is opioid use disorder and why does it matter?
- How opioid use disorder develops
- Risk factors for opioid use disorder
- Signs and symptoms of opioid use disorder
- How clinicians diagnose opioid use disorder
- Treatment options for opioid use disorder
- Living with opioid use disorder: Recovery in real life
- When to seek help (and where to start)
- Real-world experiences with opioid use disorder
- Bottom line
Not so long ago, “opioids” sounded like something that lived only in hospitals and pharmacy bottles.
Today, opioid use disorder (OUD) is a phrase most of us have heard – and for many families, it’s become painfully personal.
The good news? We understand this condition better than ever, and there are effective, evidence-based treatments that help people get their lives back.
In this guide, we’ll break down what opioid use disorder actually is, how it develops, the major risk factors, and the treatments that really move the needle
including medication options, counseling, and harm-reduction strategies. We’ll also walk through real-world experiences so this doesn’t feel like a textbook,
but a conversation about real people and real hope.
What is opioid use disorder?
Opioid use disorder is a medical condition in which a person’s use of opioids such as prescription painkillers, heroin, or fentanyl causes significant
health, social, or functional problems. It’s not just “liking pills too much.” It’s a chronic, relapsing brain disorder that changes how the brain handles
reward, stress, and self-control.
Clinicians typically use criteria from the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) to diagnose OUD. In simple terms, OUD involves
a pattern of opioid use that leads to problems like:
- Strong cravings and a persistent desire to use opioids
- Needing more of the drug (tolerance) to feel the same effects
- Withdrawal symptoms if use is reduced or stopped
- Spending a lot of time getting, using, or recovering from opioids
- Continuing to use despite harm to health, work, school, or relationships
The more criteria someone meets, the more severe the disorder is considered (mild, moderate, or severe). But here’s the key point:
OUD is treatable. It’s not a moral failure, and it’s not a lack of willpower. It’s a health condition that deserves real medical care.
How common is opioid use disorder and why does it matter?
Opioid use disorder doesn’t live in the margins of society; it cuts straight through the middle. Millions of people in the United States are estimated
to have OUD, and many more are at risk due to prescription opioid use, exposure to fentanyl in the illicit drug supply, and co-occurring mental health conditions.
Even though recent data show a promising decline in overdose deaths, opioids are still involved in the majority of fatal overdoses in the U.S.
In other words, things are improving, but we’re not done. Understanding what OUD looks like and how to treat it is still a public health priority and a personal one
for millions of families.
How opioid use disorder develops
Opioids work by attaching to receptors in the brain and body that help control pain and feelings of reward. In the short term, that can mean powerful pain relief and
a sense of euphoria and calm. Over time, repeated use can “rewire” the brain’s reward system. Instead of opioids being a choice, they start to feel like a requirement
just to function or feel “normal.”
People can develop OUD from:
- Prescription pain pills taken after surgery or injury, especially at higher doses or for longer than needed
- Nonmedical use of someone else’s prescription (for example, to “relax” or get high)
- Heroin, which is often cheaper and more accessible than prescription opioids
- Fentanyl and other synthetic opioids, which are extremely potent and often mixed into other drugs without the user’s knowledge
None of this happens overnight. For many, the journey from “my doctor prescribed this” to “my life is run by this” is gradual and often invisible to the people
around them until things get serious.
Risk factors for opioid use disorder
Not everyone who takes an opioid develops OUD. But certain risk factors raise the odds. Think of these as warning lights on the dashboard, not predictions of destiny.
Biological and genetic factors
- Family history of substance use disorders. Genetics can make some people more vulnerable to addiction.
- Brain chemistry. Differences in how the brain responds to reward and stress can make opioids feel especially compelling.
- History of other substance use. People who use alcohol, benzodiazepines, or other drugs heavily may be at higher risk.
Mental health and trauma
- Depression, anxiety, PTSD, or other mental health conditions. Opioids can temporarily numb emotional pain, making them more appealing.
- History of trauma or adverse childhood experiences. Abuse, neglect, or instability in childhood can increase risk later in life.
Medical and prescribing factors
- High-dose or long-term opioid prescriptions for pain, especially above recommended thresholds
- Use of extended-release or long-acting opioids without close monitoring
- Concurrent use of benzodiazepines (like alprazolam or clonazepam) with opioids, which raises both overdose and OUD risk
Social and environmental factors
- Living in areas with high opioid prescribing or high overdose rates
- Peer or community norms that normalize pill use or heroin use
- Unemployment, housing instability, or chronic stress
Having one or more of these risk factors does not mean someone is guaranteed to develop OUD but it does mean we should be extra careful with opioid exposure
and quick to offer support and safer options.
Signs and symptoms of opioid use disorder
OUD doesn’t come with a blinking sign, but there are patterns to watch for in yourself or someone you love. Common signs include:
- Needing larger doses of opioids to get the same effect (tolerance)
- Feeling sick, anxious, sweaty, or restless when opioids wear off (withdrawal)
- Craving opioids and spending a lot of time thinking about, getting, or using them
- Using opioids in risky situations (for example, while driving or at work)
- Continuing to use despite relationship problems, job loss, legal issues, or health scares
- Giving up activities or hobbies that used to matter
- Doctor shopping, using multiple pharmacies, or taking pills not prescribed to you
People with OUD often feel deep shame and try to hide their use. If this sounds familiar, know this: your brain is not being “dramatic” or “weak.”
It’s doing exactly what opioids trained it to do. And that can be changed with the right help.
How clinicians diagnose opioid use disorder
A diagnosis typically starts with a confidential conversation with a healthcare professional, such as a primary care doctor, addiction specialist, or psychiatrist.
They may ask about:
- What opioids you use, how much, and how often
- Any prior overdoses or withdrawal symptoms
- Other substances you use (alcohol, benzodiazepines, stimulants, etc.)
- How opioid use is affecting your life work, school, finances, relationships
- Your mental and physical health history
They then compare this information against DSM-5 criteria. Meeting two or more criteria over a 12-month period can indicate OUD, with severity grading
based on how many criteria are present. The purpose of this process isn’t to judge it’s to match you with the right level of treatment.
Treatment options for opioid use disorder
The days of telling people to “just detox and white-knuckle it” are (thankfully) fading. Modern treatment for opioid use disorder is grounded in science and
recognizes OUD as a chronic condition that often requires long-term care. The most effective approach usually includes a combination of medication, counseling,
and supportive services.
Medications for opioid use disorder (MOUD)
Three FDA-approved medications form the backbone of evidence-based treatment for OUD:
-
Methadone – A long-acting opioid agonist that prevents withdrawal, reduces cravings, and blocks the effects of other opioids.
It’s usually dispensed daily in specialized opioid treatment programs. -
Buprenorphine (often combined with naloxone) – A partial agonist that binds strongly to opioid receptors but has a “ceiling effect,”
lowering the risk of misuse and overdose. Many people know it by brand names like Suboxone®. It can be prescribed in regular medical settings by clinicians
with a standard DEA registration. -
Naltrexone – An opioid antagonist that blocks opioid receptors so opioids can’t produce a high. It’s available as a daily pill or
long-acting injection. People must be fully detoxed from opioids before starting it.
These medications:
- Reduce cravings and withdrawal symptoms
- Lower the risk of fatal overdose
- Improve chances of staying in treatment and rebuilding daily life
Staying on MOUD long term is often recommended, similar to taking medication for high blood pressure or diabetes.
Stopping too early can raise the risk of relapse and overdose, especially if tolerance has dropped.
Counseling and behavioral therapies
Medication is powerful, but it’s not the whole story. Counseling helps people understand their triggers, build coping skills, and repair relationships.
Common approaches include:
- Cognitive behavioral therapy (CBT) – Identifying thought patterns that lead to use and replacing them with healthier responses
- Motivational interviewing – Exploring ambivalence about change in a nonjudgmental way
- Contingency management – Using small, tangible rewards for staying engaged in treatment or maintaining sobriety
- Family therapy – Helping families understand OUD and rebuild trust and communication
Peer support groups (like SMART Recovery or 12-step groups) can also help many people feel less alone, though they’re most helpful when combined with medical treatment.
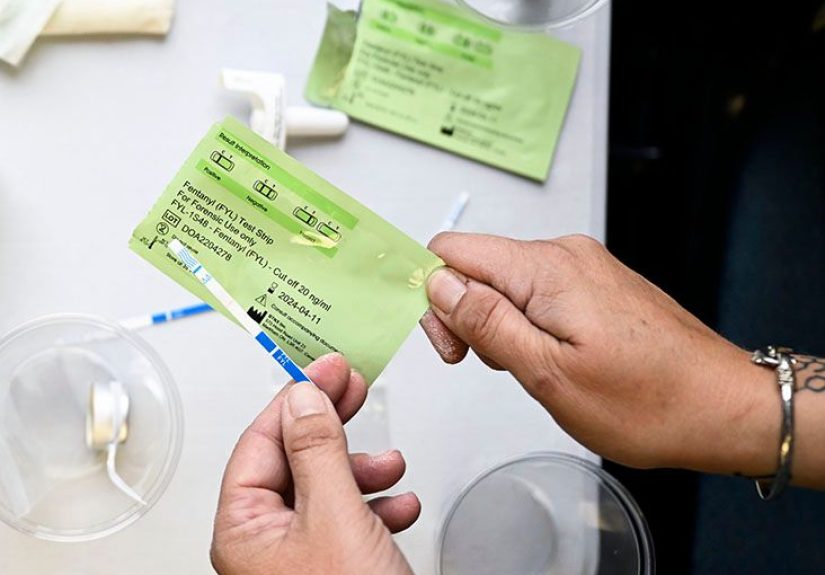
Harm reduction and overdose prevention
Harm reduction acknowledges a simple truth: people deserve to stay alive and as safe as possible even if they’re not ready or able to stop using opioids today.
Key harm-reduction strategies include:
- Naloxone (Narcan®) – A medication that quickly reverses opioid overdose. It’s increasingly available without a prescription.
- Fentanyl test strips – Tools that can detect fentanyl in street drugs so people can make safer choices.
- Never using alone – Having someone nearby who can call 911 or administer naloxone if needed.
- Safe-use education – Teaching people about mixing substances, tolerance changes after a period of abstinence, and safer dosing.
Harm reduction doesn’t “enable” opioid use. It enables survival and makes it more likely that people will live long enough to engage in treatment when they’re ready.
Levels of care and support
Treatment for opioid use disorder can look very different from person to person. Options include:
- Outpatient care with regular visits for medication and counseling
- Intensive outpatient or partial hospitalization programs with multiple sessions per week
- Residential or inpatient programs for people needing more structure and support
- Recovery housing and peer support services
The “right” level of care isn’t about what looks toughest or strictest on paper it’s about what someone can engage in consistently and safely, with the least disruption
to the life they’re trying to rebuild.
Living with opioid use disorder: Recovery in real life
Recovery from OUD rarely follows a neat, straight line. It’s usually more like a messy squiggle: progress, setbacks, restarts, and surprising moments of pride.
That’s normal. The goal isn’t perfection. It’s movement in a healthier direction over time.
Helpful strategies for living with OUD or supporting someone who has it include:
- Staying connected – Isolation feeds addiction. Supportive relationships help recovery.
- Celebrating small wins – Making it to today’s appointment or using one less pill is a meaningful step.
- Planning for rough days – Having a list of people to call, coping skills to try, and emergency resources handy.
- Accepting that lapses happen – A slip doesn’t erase progress. It signals the need to adjust the treatment plan.
Stigma can be one of the biggest barriers. Learning and talking about OUD as a medical condition not a character flaw is one of the kindest things
we can do for ourselves and others.
When to seek help (and where to start)
If you’re wondering, “Is my opioid use a problem?” that question alone is a reason to talk to someone. You don’t have to wait for an overdose, an arrest,
or a rock-bottom moment. Earlier help usually means fewer complications and better outcomes.
You can start by:
- Talking with a primary care provider or mental health professional
- Contacting a local addiction treatment program or community health center
- Reaching out to trusted friends or family and asking for help making the first appointment
If you’re in the United States and feel unsafe or at immediate risk of overdose or self-harm, call 911 or your local emergency number.
For emotional support, you can contact the 988 Suicide & Crisis Lifeline by calling or texting 988.
This article is for general education only and is not a substitute for professional medical advice, diagnosis, or treatment.
Always talk with a qualified healthcare professional about your specific situation.
Real-world experiences with opioid use disorder
Numbers and definitions are helpful, but they don’t capture what opioid use disorder actually feels like. While every person’s story is unique,
these composite experiences drawn from common patterns shared by people in recovery may sound familiar.
“It started with a legitimate prescription.”
Imagine a man in his 40s with a back injury from years of physical labor. At first, the prescription opioids are a lifesaver:
he can sleep, go to work, and play with his kids again. But as months pass, the original dose stops working as well. The doctor increases it.
On bad days, he takes an extra pill or two because “the bottle will last, it’s fine.”
When the doctor eventually tapers his dose, he starts to feel awful: flu-like symptoms, anxiety, restless legs, and a crushing sense that nothing will ever be okay again.
He doesn’t recognize these as withdrawal at first he just knows that if he takes more pills, he feels better. When prescriptions become harder to get,
a friend offers him pills from another source. Then someone mentions heroin being cheaper. None of this was the plan, but step by step, opioids have taken over.
His turning point comes after a nonfatal overdose in his driveway, with his kids inside the house. In the hospital, a clinician talks to him not like a criminal,
but like a patient with a treatable condition and offers buprenorphine. He starts medication, joins an outpatient program, and slowly regains his footing.
There are relapses, tearful conversations, and days where cravings feel loud. But month by month, he moves from “I can’t imagine life without pills”
to “I can’t believe how much life I almost missed.”
“I was using to numb everything, not just pain.”
Picture a young woman in her 20s with a history of anxiety and trauma. She’s given opioids after oral surgery and, for the first time, notices that
not only does her physical pain ease, but her mind goes quiet. No spinning thoughts. No panic. Just relief.
Later, when stress ramps up, she buys pills from classmates. Opioids become her “off switch” for overwhelming feelings.
Over time, she starts missing classes, losing weight, and pulling away from friends. When her supply dries up, withdrawal hits hard.
Her brain insists that using again is the only way to function.
She finally confides in a friend after a terrifying night of withdrawal and suicidal thoughts. The friend helps her call a crisis line and find
a program that combines MOUD with trauma-informed therapy. In treatment, she learns that her opioid use made sense in the context of her pain
but there are safer, more sustainable ways to cope. She doesn’t magically “get over it” in 30 days. Instead, she builds new habits:
going to therapy, taking buprenorphine, practicing grounding skills, and reconnecting with people who support her recovery.
“Supporting a loved one is a marathon, not a sprint.”
Families often ride their own roller coaster when a loved one has OUD. Parents may swing between anger, fear, and guilt. Partners may feel betrayed and exhausted.
It’s common to ask, “Why can’t they just stop?” or “What did I do wrong?”
One family learns, through a support group, to reframe their thinking: instead of seeing OUD as defiance or disrespect, they start seeing it as a brain disease
that is treatable but difficult to manage. They set boundaries (for example, no using in the house, no money for drugs), but they also stay emotionally available.
When their loved one finally says, “I think I’m ready for treatment,” they already have information about local programs and medications.
Along the way, the family does something crucial: they get support for themselves. They attend groups, see therapists, and learn how to balance compassion with self-care.
They can’t “fix” OUD for their loved one, but they can walk beside them and that makes a significant difference.
Why these experiences matter
These stories aren’t unusual. They mirror what many people and families face: a slow slide into opioid dependence, a series of “wake-up calls,” and eventually,
a decision to seek help sometimes more than once. They also highlight a crucial truth:
- People rarely choose opioid use disorder, but they can choose recovery, especially when real treatment is available.
- Medications for opioid use disorder are not “substituting one drug for another” they’re stabilizing brain chemistry so people can rebuild their lives.
- Supportive relationships and reduced stigma are powerful medicines in their own right.
If you see your story in any of these experiences, know that you are not alone, you are not beyond help, and you absolutely deserve care that matches the science we now have.
Bottom line
Opioid use disorder is a serious but treatable medical condition. It emerges from a mix of biology, environment, mental health, and exposure to powerful drugs in both medical
and nonmedical settings. Risk factors can help identify who needs extra care and monitoring, but no one is “hopeless” or “too far gone.”
Evidence-based treatments especially medications like methadone, buprenorphine, and naltrexone, combined with counseling and harm reduction significantly improve survival
and quality of life. Real people are reclaiming their futures every day. With accurate information, compassionate support, and access to care,
opioid use disorder doesn’t have to be the end of the story. It can be a turning point.






