Table of Contents >> Show >> Hide
- What “Type” Means (Because There Are Actually Several “Types”)
- Non-Invasive (In Situ) Breast Conditions: Early, Localized, and Often Highly Treatable
- The Most Common Invasive Breast Cancers
- Less Common (But Important) Breast Cancer Types
- Breast Cancer Subtypes by Biomarkers: The “ER/PR/HER2” Story
- How Doctors Pull It All Together: Stage, Grade, and “What’s the Plan?”
- Symptoms and Red Flags (A Quick, Practical Section)
- Questions Worth Asking Your Care Team
- Conclusion
- Experiences and Practical Perspectives (Real-World Moments That Don’t Show Up on Lab Reports)
“Breast cancer” sounds like one big, scary labellike every movie villain being called “Bad Guy.” In real life, breast cancer has many identities. Some grow slowly and stay put. Some move like they’re late for a flight. Some respond beautifully to hormone-blocking meds, while others ignore them like unread group texts.
That’s why understanding different types of breast cancer matters. Your type helps predict behavior, guides treatment, and (most importantly) turns a foggy diagnosis into something your medical team can act on with a plan. Let’s break it down in plain Englishwith just enough humor to keep your eyebrows from permanently living in the “worried” position.
What “Type” Means (Because There Are Actually Several “Types”)
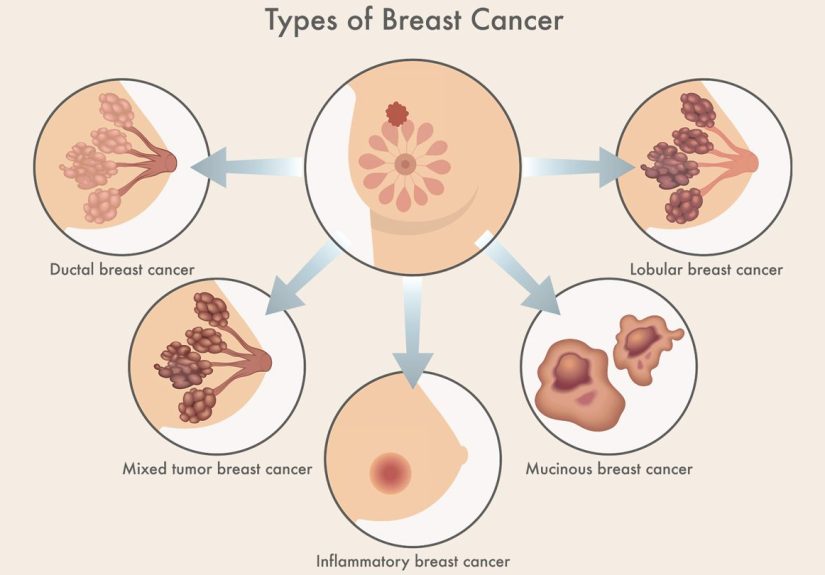
Here’s the twist: when people say “type,” they might mean one of three things: where it starts (ducts vs. lobules), how far it’s gone (in situ vs. invasive), and what it’s driven by (hormones, HER2, or neither). Think of it like describing a car: make/model (where it starts), mileage (how far it’s traveled), and engine type (what powers it).
1) Where it starts: ducts, lobules, or (rarely) other tissue
Most breast cancers begin in:
- Milk ducts (the “pipes” that carry milk to the nipple)
- Lobules (the “milk-making factories”)
Less commonly, cancers can start in connective tissue, blood vessels, or other structures in the breast. These tend to be rare and often get their own special names (more on that later).
2) In situ vs. invasive: “staying home” vs. “leaving the neighborhood”
In situ means the abnormal cells are still in the place where they startedno breaking through the wall, no moving into nearby breast tissue. Invasive means cells have moved into surrounding tissue and may spread to lymph nodes or beyond.
3) Biomarkers: ER, PR, HER2 (aka the “fuel source”)
After a biopsy, labs test the tumor for biomarkers: estrogen receptor (ER), progesterone receptor (PR), and HER2. These markers help define breast cancer subtypes and strongly influence treatment choices.
Non-Invasive (In Situ) Breast Conditions: Early, Localized, and Often Highly Treatable
Ductal Carcinoma In Situ (DCIS)
DCIS forms in the lining of a milk duct and stays containedoften called stage 0 or “non-invasive” breast cancer. DCIS is frequently found on a mammogram (sometimes before it causes any symptoms).
Why it matters: DCIS isn’t invasive yet, but some DCIS can become invasive over time. Treatment is often aimed at preventing that future plot twist. Depending on the situation, options may include surgery (like lumpectomy), sometimes radiation, and possibly hormone therapy if the cells are hormone receptor-positive.
Lobular Carcinoma In Situ (LCIS)
Despite the dramatic name, LCIS is generally considered a risk marker rather than “true cancer.” It describes abnormal-looking cells in the lobules that haven’t spread into nearby tissue.
Why it matters: LCIS increases the chance of developing breast cancer later (in either breast), so the focus is often on risk reduction and enhanced screening. Some people may discuss medications to lower risk or, in select situations, surgical prevention strategiesdecisions that are highly personal and based on overall risk factors.
The Most Common Invasive Breast Cancers
Invasive Ductal Carcinoma (IDC)
IDC starts in a duct and then breaks into surrounding breast tissue. It’s the most common form of breast cancer, making up roughly 70–80% of cases in many U.S. references.
IDC can show up in different “flavors” biologicallyhormone receptor-positive, HER2-positive, or triple-negativeso the exact treatment plan varies. In practice, many people hear “IDC” and then quickly learn the next crucial details: stage, grade, ER/PR, HER2, and lymph node involvement.
Invasive Lobular Carcinoma (ILC)
ILC begins in the lobules and invades nearby tissue. Compared with IDC, it can be trickier to spot because it may not form a neat, obvious lump. Sometimes it spreads in a subtle, “sneaky vine” pattern through breast tissue.
Clinically, that can influence imaging choices and surgical planning. Many ILC tumors are hormone receptor-positive, but as always, testing is what tells the truthnot vibes.
Less Common (But Important) Breast Cancer Types
Inflammatory Breast Cancer (IBC)
Inflammatory breast cancer is rare and fast-growing. It often doesn’t announce itself with a classic lump. Instead, it may cause redness, swelling, warmth, skin thickening, or a dimpled “orange peel” texture (yes, medicine truly has a phrase for everything: peau d’orange).
IBC happens when cancer cells block lymph vessels in the skin of the breast, creating an inflamed appearance. Because it can mimic infection, persistent symptomsespecially if antibiotics don’t helpshould be evaluated promptly.
Paget Disease of the Breast (Paget Disease of the Nipple)
Paget disease involves the nipple (and often the areola) and may look like eczema: flaky, crusty, irritated skin or discharge. It’s uncommon, but it’s important because it’s often associated with an underlying DCIS or invasive breast cancer deeper in the breast.
Translation: if a “nipple rash” isn’t improving or keeps returning, it deserves a proper medical looknot just a new tube of ointment and wishful thinking.
Metastatic Breast Cancer (Stage IV)
Metastatic breast cancer means cancer has spread beyond the breast and nearby lymph nodes to other parts of the body (commonly bone, liver, lungs, or brain). Sometimes it’s metastatic at first diagnosis (called de novo stage IV), and other times it develops after earlier-stage treatment.
While stage IV is serious, treatment options have expanded dramatically over time, especially with targeted therapies guided by biomarkers. The goal is often long-term controlmore like managing a chronic condition than a short sprint.
Rare Histologic Types (The “Special Editions”)
Some breast cancers are defined by how they look under the microscope. Examples include: tubular, mucinous (colloid), papillary, and other uncommon patterns. There are also rare tumors arising from different tissues, like angiosarcoma (from blood/lymph vessels).
These are less common, but they matter because behavior and treatment can differ from standard IDC/ILC. If your pathology report includes a rare subtype, it’s reasonable to ask whether a breast cancer specialist or tumor board review is recommended.
Male Breast Cancer
Men can get breast cancer, too. It’s rare, so awareness is lower, which can delay evaluation. Symptoms can include a lump, nipple changes, or discharge. Biology and treatment principles are similar, but care should be tailored to the individual.
Breast Cancer Subtypes by Biomarkers: The “ER/PR/HER2” Story
Two people can both have “IDC,” but their cancers may behave very differently depending on biomarkers. That’s why modern care often centers on breast cancer subtypes such as hormone receptor status and HER2 status.
Hormone Receptor-Positive (ER+ and/or PR+)
Hormone receptor-positive breast cancer means the tumor cells have receptors for estrogen and/or progesterone. In many cases, these cancers can respond well to hormone (endocrine) therapy that blocks hormone signaling or reduces hormone production.
People sometimes hear “hormone-positive” and assume it’s automatically “easy.” Not exactly. It often has effective long-term options, but treatment can be a marathon, sometimes including years of endocrine therapy.
HER2-Positive
HER2-positive breast cancer means tumor cells have too much HER2 protein or extra HER2 gene activity, which can promote faster growth. The key upside: HER2 is a target, and targeted therapies have significantly changed outcomes for many patients.
HER2-positive cancers can also be hormone receptor-positive (sometimes called “triple-positive” if ER+, PR+, HER2+), which may open the door to both HER2-targeted therapy and hormone therapy, depending on the clinical scenario.
Triple-Negative Breast Cancer (TNBC)
Triple-negative breast cancer means the tumor lacks ER, PR, and doesn’t have high HER2. Because it doesn’t use those pathways, hormone therapy and HER2-targeted drugs won’t help.
TNBC can be more aggressive and may rely heavily on chemotherapy and, in certain settings, immunotherapy or other targeted approaches. It’s also more likely to be associated with BRCA-related biology in some patients, so genetic counseling/testing may be discussed depending on age, family history, and other factors.
How Doctors Pull It All Together: Stage, Grade, and “What’s the Plan?”
If your diagnosis feels like a bowl of alphabet soup (DCIS! IDC! ER! PR! HER2!), here’s the organizing principle: doctors combine type, stage, grade, and biomarkers to choose the most effective treatment with the least unnecessary chaos.
Staging (0–IV): Where it is and where it isn’t
Staging often uses the TNM system: T (tumor size), N (lymph node involvement), and M (metastasis). Stage 0 includes in situ disease like DCIS. Stages I–III are localized/regionally advanced to varying degrees. Stage IV means distant spread.
Important: stage is not “how bad of a person you’ve been.” It’s not karma. It’s anatomy.
Grade: How “rowdy” the cells look
Grade describes how abnormal the cancer cells appear compared to normal cells and how quickly they may be growing. A higher grade can suggest a faster-growing tumor, which may influence treatment intensity.
Examples of how type changes treatment choices
- DCIS: Often surgery-focused, sometimes radiation, and endocrine therapy may be considered if hormone receptor-positive.
- ER+/PR+: Endocrine therapy can be a cornerstone, sometimes combined with surgery, radiation, and/or chemo depending on stage and risk.
- HER2+: HER2-targeted therapy is often central, paired with surgery and possibly chemo/radiation depending on stage.
- TNBC: Often chemo-forward; in certain cases, immunotherapy may be part of the plan.
- IBC: Typically requires urgent, multi-step treatment (systemic therapy first is common), plus surgery and radiation planning.
Symptoms and Red Flags (A Quick, Practical Section)
Not everyone has symptoms (screening mammograms catch many cancers early), but common red flags include:
- A new lump or thickening in the breast or underarm
- Nipple discharge (especially bloody) or nipple inversion that’s new
- Skin changes: dimpling, puckering, persistent redness, swelling, warmth
- A rash or flaky skin on the nipple/areola that doesn’t resolve
- One breast suddenly looks different in size/shape
If something feels off and it persists, get it checked. You are not “being dramatic.” You are being appropriately attentive to a body part with a surprisingly complicated résumé.
Questions Worth Asking Your Care Team
Appointments can be overwhelming, so consider keeping a short list:
- What is the exact type (IDC, ILC, DCIS, IBC, etc.) and what does that imply?
- What are the biomarkers (ER, PR, HER2)? Is it triple-negative or HER2-positive?
- What stage and grade is it? Are lymph nodes involved?
- What are the main treatment goals (cure, long-term control, symptom management)?
- Should I consider genetic counseling/testing based on my situation?
- Would a second opinion or tumor board review be helpful?
- What side effects should I expectand what can we do to prevent or reduce them?
Conclusion
Understanding different types of breast cancer is less about memorizing medical vocabulary and more about gaining clarity. The “type” can refer to where it started (ducts or lobules), whether it’s invasive, and what biomarkers it carries (ER/PR/HER2). Those details shape treatment, help predict behavior, and turn uncertainty into a tailored strategy.
If you’re navigating diagnosis or supporting someone who is, remember this: you don’t need to become an oncologist overnight. You just need enough knowledge to ask good questions, understand the plan, and advocate for care that fits the cancer in front of you. (And yes, it’s okay to bring a notebook. Or a friend. Or both. Cancer doesn’t get to be the only one taking notes.)
Experiences and Practical Perspectives (Real-World Moments That Don’t Show Up on Lab Reports)
Medical definitions are useful, but lived experience adds contextespecially when the words “type” and “subtype” start piling up faster than laundry. Here are common experiences people report when learning about different breast cancer types, along with practical takeaways. These are not one person’s story; they’re patterns that show up again and again in clinics, support communities, and conversations over coffee that gets cold because nobody remembers to drink it.
The “Wait, I Thought It Was Just One Thing” Moment
Many people start with a simple assumption: breast cancer is breast cancer. Then pathology results arrive with acronyms: IDC, ER+, HER2-, maybe a Ki-67 number, and suddenly it feels like your body enrolled itself in a graduate program without telling you. A helpful coping trick is to ask your clinician to summarize your diagnosis in one sentence, then build from there. Example: “This is invasive ductal carcinoma, stage II, ER/PR positive, HER2 negative.” That single sentence becomes your anchor.
DCIS: Relief, Then Confusion
People diagnosed with DCIS often describe a strange emotional whiplash. “It’s stage 0” can sound reassuringuntil the word “carcinoma” lands. A common experience is wondering: “If it’s not invasive, why do I need surgery?” The practical answer is that treatment often focuses on preventing a future invasive cancer. Many find it empowering to ask about their specific DCIS features (grade, size, margins, hormone receptor status) and how those influence recurrence risk and treatment options.
ILC: When Imaging Feels Like a Treasure Hunt
People with invasive lobular carcinoma (ILC) sometimes describe extra imaging or “we’re double-checking” appointments. Because ILC can grow in a more diffuse pattern, it may not always form a clear, round lump. The experience can feel frustratinglike the tumor is playing hide-and-seek with very expensive equipment. If this happens, it can help to ask what imaging is best for your case and how the team will make sure surgery targets the right area.
IBC: “But It Looks Like a Rash…”
People who end up diagnosed with inflammatory breast cancer often report being surprised because the symptoms can resemble infection: redness, swelling, warmth, skin texture changes, tenderness. A recurring theme is wishing they’d known earlier that a persistent “breast rash” that doesn’t improve deserves a prompt evaluation. The practical takeaway: if you see fast changes (especially on one side) that don’t resolve, don’t self-manage indefinitely. Getting the right diagnosis quickly matters with IBC.
Biomarker Emotions: When “Triple-Negative” Sounds Like a Villain Name
People hearing triple-negative breast cancer (TNBC) for the first time often describe fearbecause it sounds like “nothing works.” In reality, it means hormone therapy and HER2-targeted therapies aren’t a match, but other treatments can be effective and are improving. The practical move is to ask, “What treatments work best for this subtype at my stage?” (Stage matters a lot.) Many also find it grounding to focus on the plan: the sequence of treatment, the goal, and what “response” will be measured.
Support Systems: The Quiet Superpower
Across typesDCIS, IDC, HER2+, TNBC, metastaticpeople consistently report that support isn’t a luxury; it’s part of the treatment ecosystem. Sometimes support is a partner who shows up to appointments. Sometimes it’s a group chat that sends memes at 2 a.m. Sometimes it’s a therapist who helps you remember you are still you, not just a diagnosis with paperwork. A practical suggestion: choose one person to be your “information buddy”someone who can take notes, track questions, and help you interpret the plan when your brain is understandably tired.
The bottom line: the “type” of breast cancer is a medical classification, but the experience is human. Clarity helpsso keep asking questions until the words on the report turn into a plan you understand. And if humor helps you breathe a little easier, use it. You’re allowed to laugh, even while being very, very serious about your health.